Current Smoking vs Cancer: Why the Correlation Is Modest
Current smoking and lung cancer still move in the expected direction at the county level, but the relationship is only moderate. That is what we would expect when recent survey data are being compared with cancers caused by older exposures, and when counties differ on many other health and social factors at the same time.
What is r?
Pearson r measures the direction and strength of a straight-line relationship. Positive means higher smoking tends to go with higher cancer; negative means the opposite.
What is R²?
R² is the share of county-to-county variation captured by the trend line. R² = 0.14 means smoking alone captures 14% of the differences between counties in this specific dataset.
What is the p-value?
The p-value asks how surprising this pattern would be if the true county-level relationship were zero. Smaller p-values mean the pattern is harder to dismiss as random noise.
Significant vs not
Here, p < 0.05 is labeled statistically significant. That is evidence of a pattern in this dataset, not proof of causation. "Not significant" is not the same as "no effect."
Current smoking (WTN BRFSS 2020–22) vs lung cancer incidence rate (WTN 2016–20). Hover over dots for county details. Highlighted counties are notable outliers. Several county smoking estimates come from relatively small BRFSS samples, and some are flagged NR, which adds noise to this plot. (Washington State Department of Health, n.d.-a, n.d.-d)
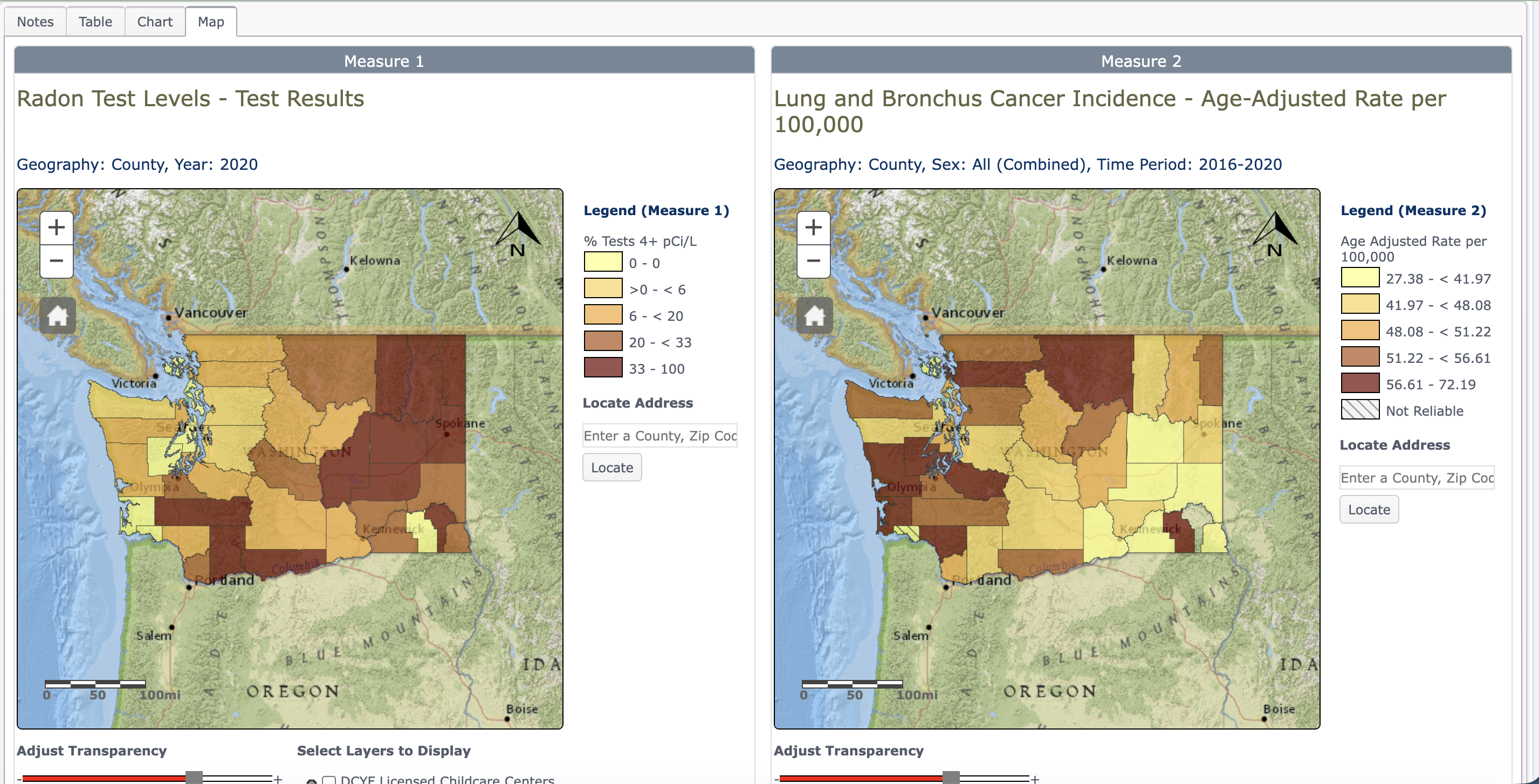
A map view makes the same county pattern easier to read spatially: current smoking is highest across several rural inland counties, while the lung cancer map stays elevated in parts of the southwest coast and interior. The overlap is real, but it is not perfectly one-to-one. (Washington State Department of Health, n.d.-a, n.d.-d)
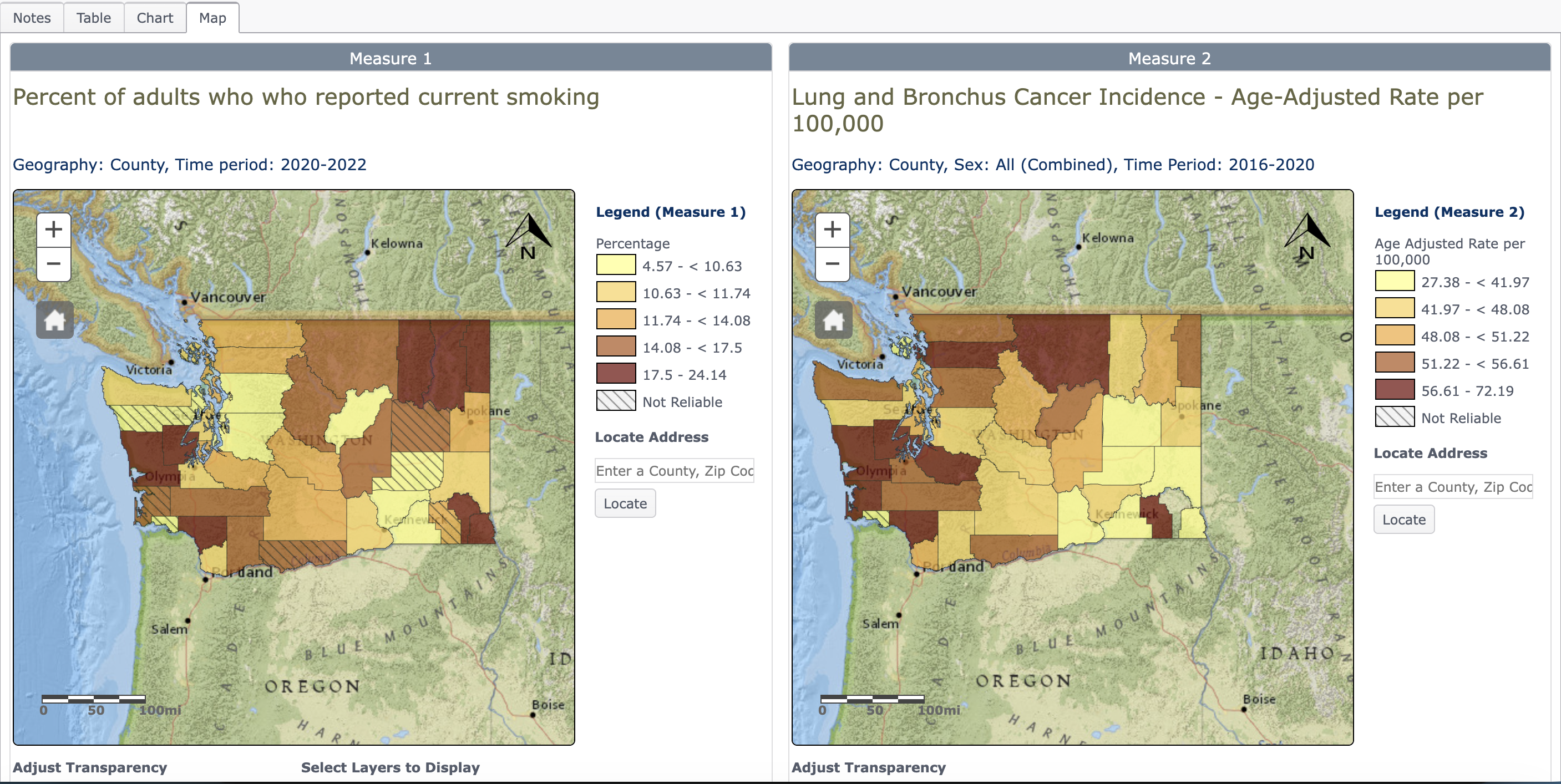
Side-by-side county maps from the Washington Tracking Network comparing current smoking estimates with lung cancer incidence.
What the numbers mean in plain English: Counties with more current smokers do tend to have more lung cancer, but the scatter is still wide. R² = 0.14 means current smoking does not explain most of the county-to-county differences by itself.
Why p = 0.024 matters: If there were truly no county-level relationship at all, a pattern at least this strong would show up by chance only about 2.4% of the time. That clears the usual 5% cutoff for statistical significance.
Why the fit is still modest: Lung cancer takes 15–30 years to develop after smoking exposure, so the 2020–22 survey does not line up with the most relevant exposure years for cancers diagnosed in 2016–2020. County-level results are also diluted by survey noise, occupational exposure, healthcare access, and demographic differences. A moderate ecological correlation is therefore still consistent with smoking being the main causal driver of lung cancer.